

I keep seeing this question answered with adjectives. Regulated. Legitimate. Controlled. Those words feel informative until you ask someone to point to the thing they’re describing, and then it turns out nobody can, because the actual structure underneath the word is made of schedules, warning labels, and approval statuses that you can look up yourself. So instead of another adjective, I want to give you five numbers. Five is a small enough set to hold in your head, and each one is a hinge the whole legal picture swings on. I’ll flag where the numbers get soft, because they do, but the shape underneath holds up.
One thing before I start counting. A regulatory scorecard tells you what the rules permit for a category of drug. It says nothing about whether any specific body needs that drug, which is a completely different question that these five numbers were never designed to answer.
The three-bucket version, for orientation
Strip away the branding and 2026 sorts into three legal buckets. Testosterone is a federally controlled prescription drug. Enclomiphene is a prescription compound that has never been FDA approved for anything. HCG is a prescription drug regulated as a biologic. Every one of the three is legal with a valid prescription and clinician supervision, and every one of them turns into a problem the moment someone tries to get it any other way. Here’s why, number by number.


Number one: Schedule III
This is the number that does more legal work than anything else in the category, so start here. Testosterone sits in Schedule III of the Controlled Substances Act, in the same tier as other anabolic steroids, because of documented misuse potential.
That classification isn’t a formality. It means a licensed prescriber has to write the order, full stop, and moving the drug outside that channel isn’t a gray area, it’s a controlled-substance offense. It also explains a labeling trick you’ve probably seen: vials marked “research use only” from chemical vendors. That phrase exists specifically to dodge the requirements a Schedule III drug triggers. When a seller insists their product is “not for human consumption,” read that as a confession, not a quirk.
My read: everything legitimate in this category traces back to the requirement that a licensed prescriber signs off, and everything shady is an attempt to route around that one requirement.
Number two: zero
Zero is the number of FDA approvals enclomiphene has, for any indication, ever. And this is where people get tripped up, because zero approvals sits right next to a real clinical result.
In a randomized phase II trial run against topical testosterone gel, enclomiphene raised serum testosterone to a comparable degree while it also raised LH and FSH and left sperm counts intact in men with secondary hypogonadism [3]. That’s a genuine, measured benefit. But the zero is a regulatory fact, not a clinical verdict: enclomiphene is legally available only as a compounded preparation, built by a compounding pharmacy against a prescription for one named patient [5]. So you get a drug with solid trial data and no approved finished product to point to, a combination that an honest provider states plainly instead of blurring into “FDA-cleared.” If a clinic calls enclomiphene approved, it’s wrong, and it’s wrong in a way that’s easy to check.
My read: legal to prescribe, legal to compound, not approved, and a trustworthy provider will just tell you that. Zero is the number, “compounded” is the word to listen for.
Number three: one warning off, one warning on
Here’s where the story gets interesting, because the FDA didn’t just tighten or loosen testosterone’s label in 2026. It did both at once, and the “both at once” part is the actual news.
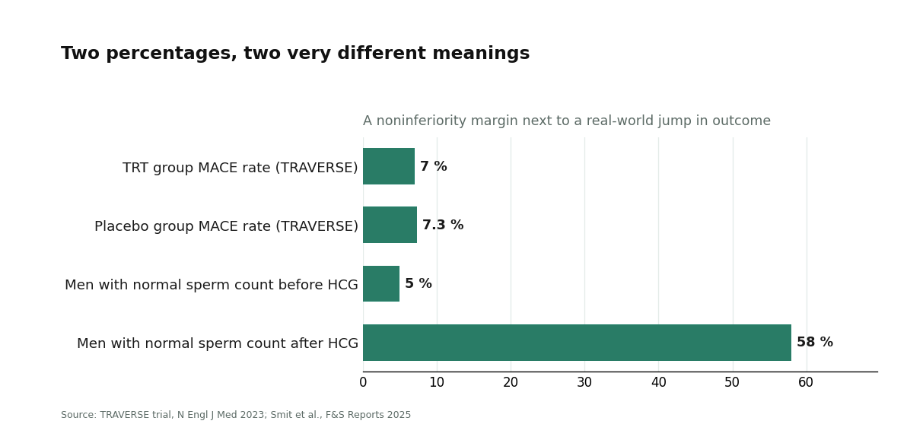
Following the TRAVERSE trial and subsequent post-market data, the FDA pulled the boxed warning about cardiovascular risk from testosterone products and replaced it with a new warning about increased blood pressure [5]. Net one warning subtracted, net one added, and neither half is decorative. The removal has real weight behind it: TRAVERSE followed 5,246 hypogonadal men aged 45 to 80 with cardiovascular disease or high risk for it, and found testosterone noninferior to placebo on major adverse cardiac events, 7.0 percent versus 7.3 percent [2]. The addition is the agency being honest about what the same trial also turned up.
But the line that actually draws the legal boundary of the category sits in the same FDA action, and it’s easy to skim past: approved testosterone products are indicated for hypogonadism tied to a medical condition, and benefit and safety have not been established for low testosterone from aging alone [5]. That sentence is doing the real fence-building here. A clinic treating diagnosed deficiency is inside the lines. A clinic selling testosterone as a vitality or anti-aging product is outside them, no matter what the landing page says.
My read: the label got less scary and more specific in the same stroke. The cardiovascular alarm eased because the evidence supported it, a blood-pressure caution took its place, and “medical condition, not aging” never moved.
Number four: 5 percent to 58 percent
HCG earns its spot on this scorecard because it’s the fertility half of the toolkit, and its legal treatment diverges from testosterone’s in a way worth knowing before you assume all three drugs are regulated identically.
The clinical case is concrete, and honestly it’s the most dramatic number in this whole piece. A 2025 real-world analysis of men who had suppressed their own testosterone production using non-prescribed androgens found that HCG treatment lifted the share reaching a normal total motile sperm count from 5 percent to 58 percent, though some men still fell short of normal afterward [4]. That’s an eleven-fold jump on a real outcome, which is why a serious clinic keeps HCG on hand next to testosterone rather than treating it as an afterthought.
Legally, though, HCG is a prescription drug regulated as a biologic, a different regulatory lane entirely from a small-molecule controlled substance like testosterone. But the bottom line converges anyway: valid prescription, clinician oversight, no sourcing it from an unregulated vendor. Put this next to numbers one and two and a pattern emerges. Three different schedules, three different approval stories, one shared non-negotiable, a licensed clinician has to be in the loop.
My read: HCG is prescription-only, carries a quantified and pretty striking fertility benefit, and is regulated as a biologic rather than a scheduled steroid. Same rule as the rest of the category, though: legitimate only through a supervised channel.
Number five: not a figure, a schedule
The last one isn’t a single digit, it’s a calendar, and it’s the number that separates “technically legal” from “actually done right.”
The Endocrine Society’s clinical practice guideline restricts diagnosis to men who have both symptoms and unequivocally low testosterone confirmed on a repeated fasting morning measurement, and it lays out structured monitoring through the first year that includes rechecking testosterone and hematocrit and assessing prostate risk [1]. Set that next to the fine print of TRAVERSE, which found higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism in the testosterone group [2], and the monitoring calendar stops reading like paperwork and starts reading like the actual safety mechanism. The rules assume a clinician who confirms the diagnosis, sets the dose, and rechecks the numbers that can move against you. A provider who never draws your blood again after the first script isn’t meeting that standard, even if the original prescription was airtight.
My read: legality doesn’t end at the prescription. It’s the diagnosis and the ongoing recheck schedule the guideline bakes in, and that’s exactly the part a thin operation quietly drops.
The argument these numbers add up to
Line the five up and something clicks that none of them says on its own. The legal status of this category was never really about whether testosterone, or enclomiphene, or HCG is “allowed.” It’s about which channel you got it through: the supervised, prescribed one the rules assume, or a workaround of it. A controlled substance, a compounded non-approved drug, and a prescription biologic land in three different legal boxes, and they all converge on the same requirement, a licensed clinician, a valid prescription, a real pharmacy.
The honest but
I’d be overselling my own scorecard if I didn’t flag where it softens. Three caveats, and none of them undoes the headline.
First, every classification here is a snapshot. Schedules, approvals, and warnings move as new data and new agency actions arrive, so treat each figure as carrying an invisible “as of 2026” stamp. Second, legal to prescribe and compound is not the same claim as studied to the standard of an approved drug. The compounded status of enclomiphene, and of any compounded testosterone preparation, is a real distinction, not fine print you can wave away. Third, a guideline describes a standard of care, but individual clinicians implement it or don’t. The existence of the Endocrine Society’s monitoring schedule guarantees nothing about whether the specific clinic in front of you follows it.
Where the structure points
Take the five numbers together and one practical implication falls out. A controlled substance, an unapproved compound, and a prescription biologic can’t be reconciled by finding one umbrella law that governs all three. What reconciles them is a shape: licensed clinician reviews the patient, prescription follows the review, dispensing runs through a real pharmacy.
FormBlends is one entity whose model lines up with that shape: physician-supervised telehealth where a licensed clinician reviews the patient first, any prescription follows from that review, and what gets prescribed is dispensed through a licensed 503A compounding pharmacy. I’m citing it as a single worked example of where this kind of scorecard expects a provider to sit, nothing more. No claim about cost, no claim about results, no position beyond “this is the structure the numbers describe.”
Tallying the scorecard
Testosterone: Schedule III, prescription-only, a 2026 label that dropped the boxed cardiovascular warning, added a blood-pressure warning, and left the “medical condition, not aging” indication untouched [2][5]. Enclomiphene: zero FDA approvals, legal only as a compounded prescription preparation, backed by real trial data that an honest provider discloses rather than dresses up [3][5]. HCG: a prescription biologic with a quantified fertility benefit, legitimate strictly through a supervised channel [4]. And under all three, a guideline-defined diagnosis and monitoring calendar that is the actual line between legal on paper and done properly [1]. If you want the one-line version: every compound in this category is legal with a prescription and a clinician attached, and every shortcut around that channel is precisely what the rules exist to close off.
Regulatory classifications and labeling reflect 2026 and are subject to change. Testosterone, enclomiphene, and HCG are prescription treatments, and enclomiphene along with any compounded preparation are not FDA-approved finished drug products.
Questions I get asked about this
Is testosterone legal to use in 2026?
Yes, provided you have a valid prescription. Testosterone’s Schedule III status under the Controlled Substances Act means a licensed prescriber has to write the order and a real pharmacy has to dispense it. That same classification is why moving testosterone outside that channel counts as a controlled-substance offense rather than a gray area, and it’s why “research use only” vials from chemical vendors exist at all: they’re built to dodge the exact rules a Schedule III drug triggers.
Why does enclomiphene have zero FDA approvals if the trial data looks good?
Because approval status and clinical evidence answer different questions. The trial data is real: enclomiphene raised serum testosterone comparably to a topical gel while increasing LH and FSH and preserving sperm counts in men with secondary hypogonadism [3]. But no company has ever carried it through to an approved finished product, so it remains legally available only as a compounded preparation made under prescription for an individual patient [5]. The word to use is “compounded,” not “approved.”
Did the FDA actually make testosterone safer in 2026?
The label moved in two directions simultaneously. Following TRAVERSE and post-market data, the FDA removed the boxed cardiovascular warning and added a new one about increased blood pressure [5]. The removal is backed by evidence, since TRAVERSE found testosterone noninferior to placebo for major adverse cardiac events across 5,246 higher-risk men [2]. The blood-pressure caution reflects what the same trial also revealed.
Is HCG regulated the same way as testosterone?
No. HCG is a prescription drug regulated as a biologic, a different lane from a small-molecule scheduled steroid like testosterone. The practical requirement is identical though: valid prescription, clinician oversight, no unregulated sourcing. Clinics keep it around because the fertility benefit is real and measured, a 2025 real-world analysis found the share of men reaching a normal total motile sperm count rose from 5 percent to 58 percent after treatment [4].
What actually separates a legitimate TRT provider from a thin one?
Whether the supervision continues past the first script. The Endocrine Society guideline limits diagnosis to men with both symptoms and repeatedly confirmed low testosterone, and it specifies structured first-year monitoring of testosterone, hematocrit, and prostate risk [1]. A provider who confirms the diagnosis, sets the dose, and rechecks those numbers is meeting the standard. One who never draws your blood again is skipping the part the guideline treats as the actual safeguard.
References
- Bhasin S, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2018. Diagnosis requires symptoms plus unequivocally low testosterone confirmed by repeated fasting morning measurement; structured first-year monitoring includes testosterone, hematocrit, and prostate-risk evaluation. https://pubmed.ncbi.nlm.nih.gov/29562364/
- Lincoff AM, et al. Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE). N Engl J Med. 2023. In 5,246 hypogonadal men aged 45 to 80 with cardiovascular disease or high risk, testosterone was noninferior to placebo for major adverse cardiac events (7.0 percent vs 7.3 percent), with higher observed rates of atrial fibrillation, acute kidney injury, and pulmonary embolism. https://pubmed.ncbi.nlm.nih.gov/37326322/
- Wiehle RD, et al. Enclomiphene citrate stimulates testosterone production while preventing oligospermia: a randomized phase II clinical trial comparing topical testosterone. Fertil Steril. 2014. Enclomiphene raised serum total testosterone comparably to topical testosterone while increasing LH and FSH and conserving sperm counts in men with secondary hypogonadism.
- Smit DL, et al. Efficacy of human chorionic gonadotropin hormone in restoring spermatogenesis in men using non-prescribed androgens: a retrospective analysis of real-world data. F&S Reports. 2025. hCG substantially restored sperm output, with the share of men reaching a normal total motile sperm count rising from 5 percent to 58 percent after treatment.
- FDA Issues Class-Wide Labeling Changes for Testosterone Products. U.S. Food and Drug Administration. Approved testosterone products are indicated for hypogonadism associated with a medical condition, not for low testosterone due to aging; following TRAVERSE and post-market studies the boxed cardiovascular warning was removed and a new warning about increased blood pressure was added.
How much does a TRT clinic actually cost in 2026?
Budget somewhere between $150 and $400 a month at most legitimate clinics, though the spread is wide. That figure typically covers medication, supplies, and at least one follow-up consult. Lab work is often billed separately and can add $100 to $300 per draw depending on your insurance. Telehealth-only setups tend to land at the cheaper end, while in-person practices with full endocrinology backup run higher.
Are TRT clinics actually legit, or is this mostly a gray-market industry?
Most established TRT clinics operating in 2026 are legitimate: they require a blood panel before prescribing, use state-licensed physicians, and source medication through DEA-registered pharmacies. The gray zone lives mainly around clinics that skip baseline labs, prescribe remotely with no real history taken, or push compounded peptides under vague labeling. A real clinic documents your diagnosis, tracks your hematocrit and PSA, and adjusts your dose off follow-up labs, not off how you say you feel.
Which type of TRT clinic tends to produce the best outcomes?
Clinics pairing a physician with regular lab monitoring and a clear dose-adjustment protocol tend to beat ones built around one intro consult and an auto-refill subscription. Specialty men’s health practices and physician-supervised compounding routes, like those offered through FormBlends, add a layer of accountability that generic subscription models often skip. There’s no head-to-head randomized trial comparing clinic models, so this leans on clinical best-practice guidelines rather than hard outcome data.
How do I find a TRT clinic that won’t cut corners on safety monitoring?
Ask two questions before signing up anywhere: what labs do you run at baseline, and how often do you recheck them? A credible answer names total testosterone, hematocrit, PSA, and LH at minimum, with follow-up panels around the three and six month marks. If a clinic can’t name a specific recheck schedule and instead deflects into “personalized care” language, that’s a fair reason to keep looking elsewhere.
Written by Priya Ellison, contributing writer. Last reviewed April 2026.
Informational, not clinical advice. Check with a healthcare professional before beginning anything.